



Ishanu Chattopadhyay PRO
ML | Data Science Biomedical Informatics | Social Science | Assistant Professor
ZPAN
Ishanu Chattopadhyay, PhD
Assistant Professor of Internal Medicine
Institute of Biomedical Informatics
University of Kentucky
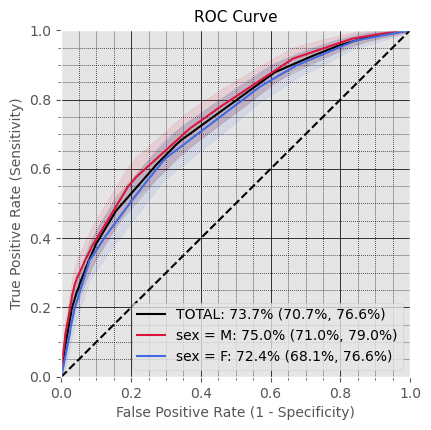
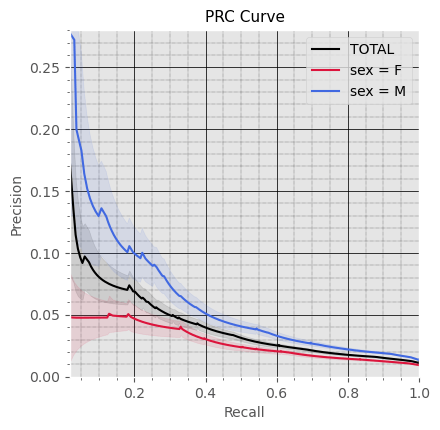
Subproblem 1
Prediction of first AP Diagnosis
Inclusion Criteria:
35-65 years old patients with >= 2 years of records available
Exclusion Criteria:
Patients with any Drug- or Alcohol-Induced Acute Pancreatitis (K85.2, K85.3) are excluded.
Prediction Target: Acute Pancreatitis (except for drug- and alcohol-induced A.P. (K85, K85.0, K85.1, K85.8, K85.9)
Time of Prediction: Case: 6 to 18 months before first target Dx; Control: 2 years before end of records
Observation window: 1 to 2 years leading to the time of prediction
Prediction Objective: Predict if any Target diagnosis will be recorded within 6 to 18 months following the time of prediction
Cohort Size:
Case: 46,135 (0.8%), Control: 5,586,388 (99.2%)
Males: 2,513,756 (44.6%), Females: 3,118,767 (55.4%)
Mean age at the time of prediction: 50 years 4 months
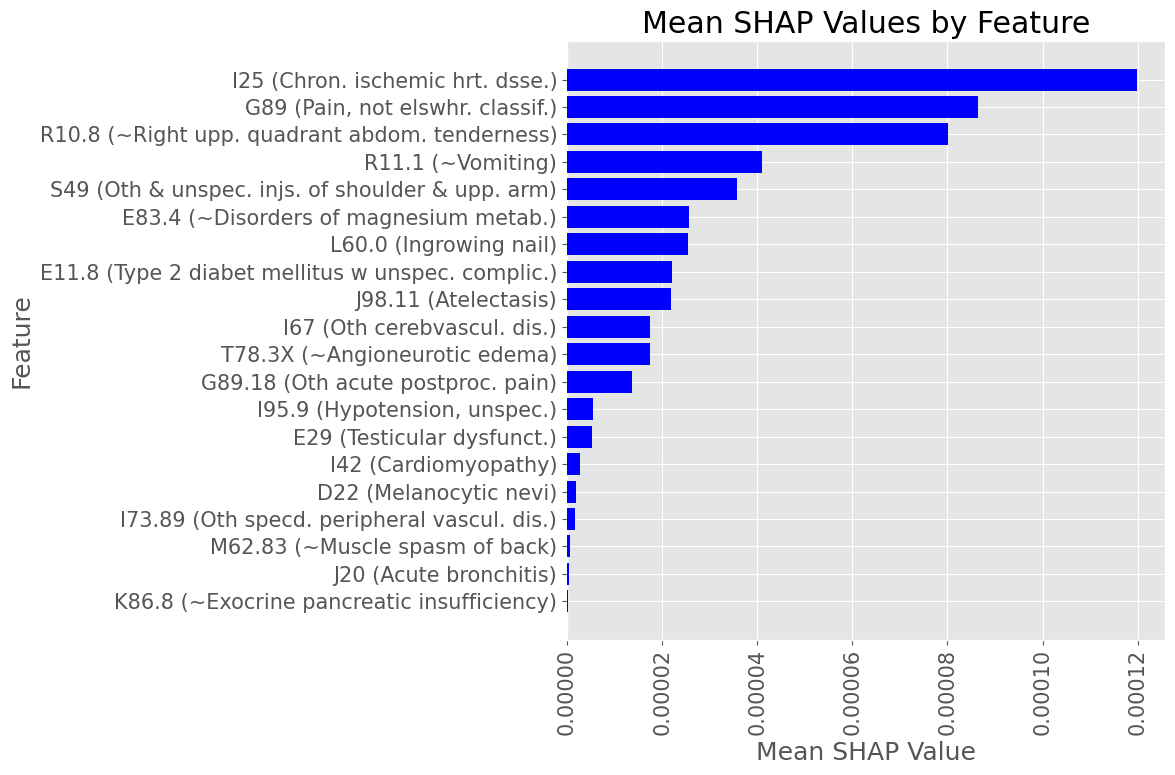
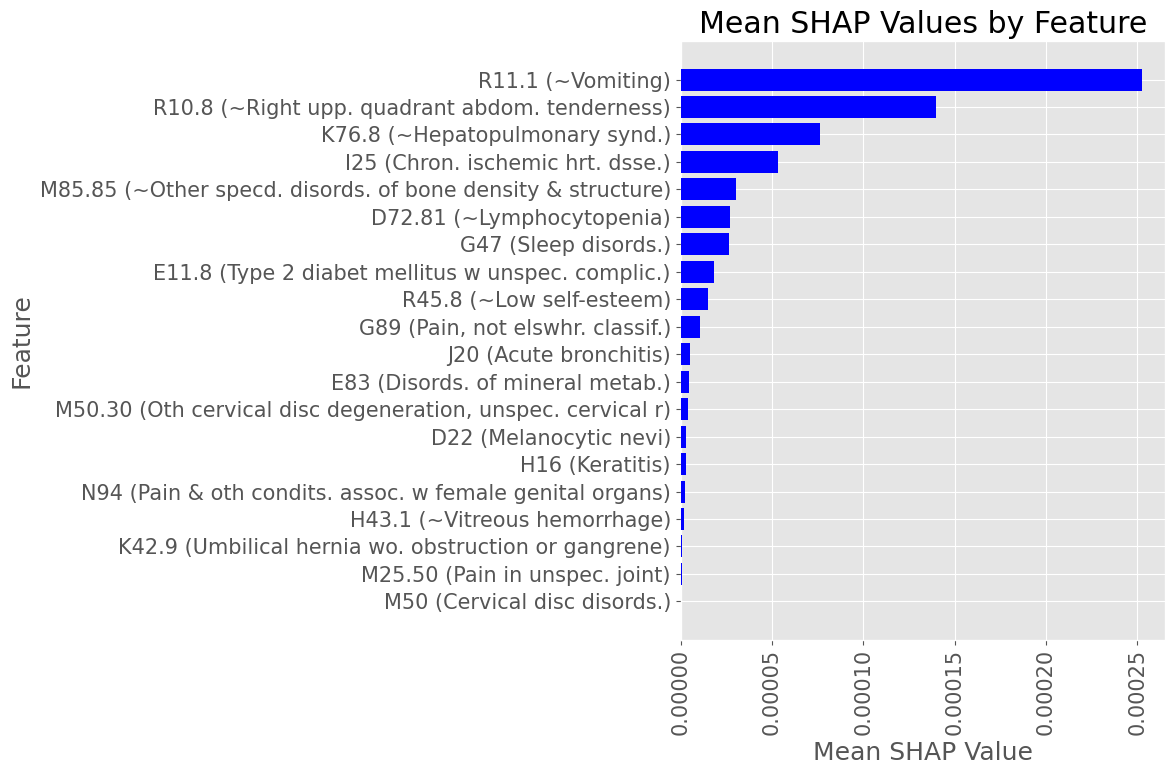
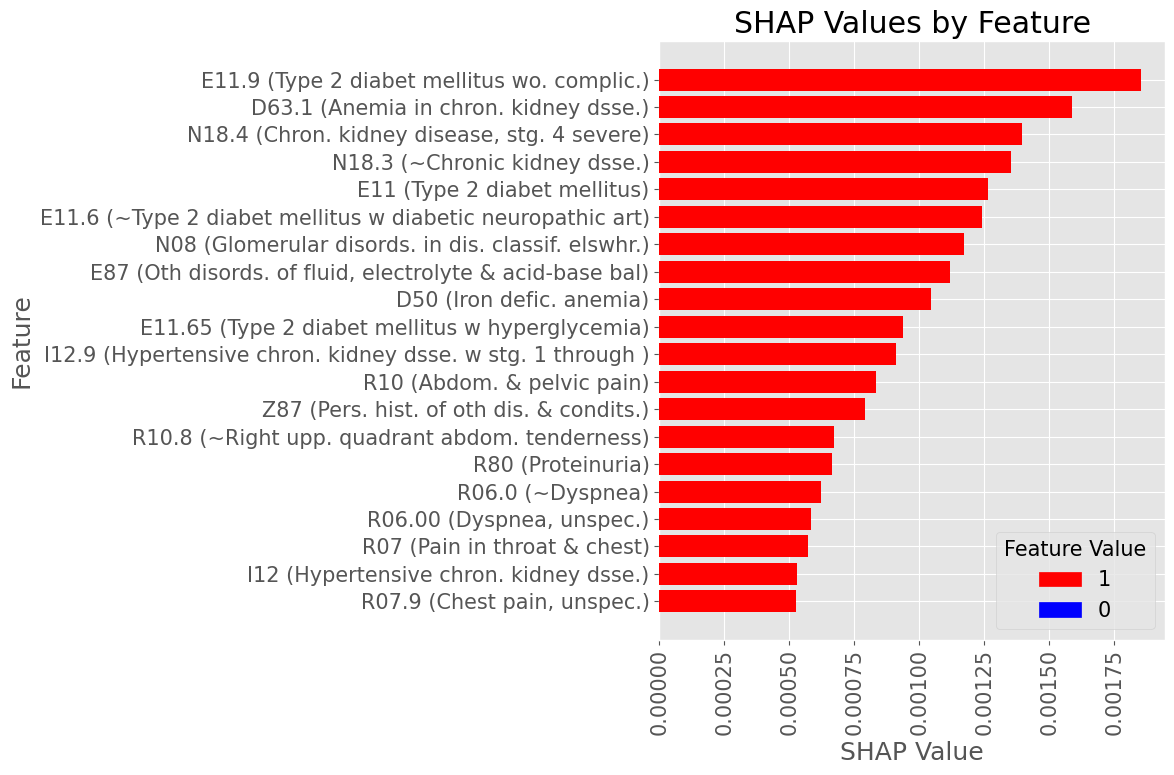
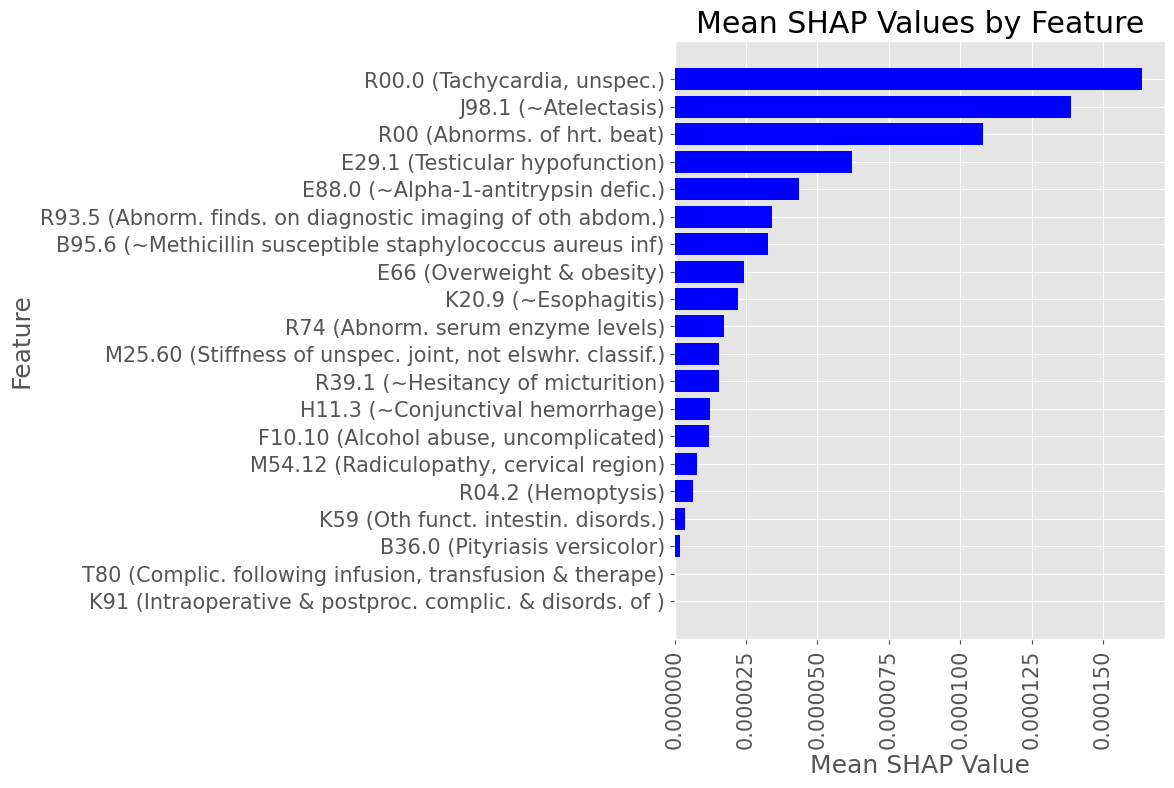
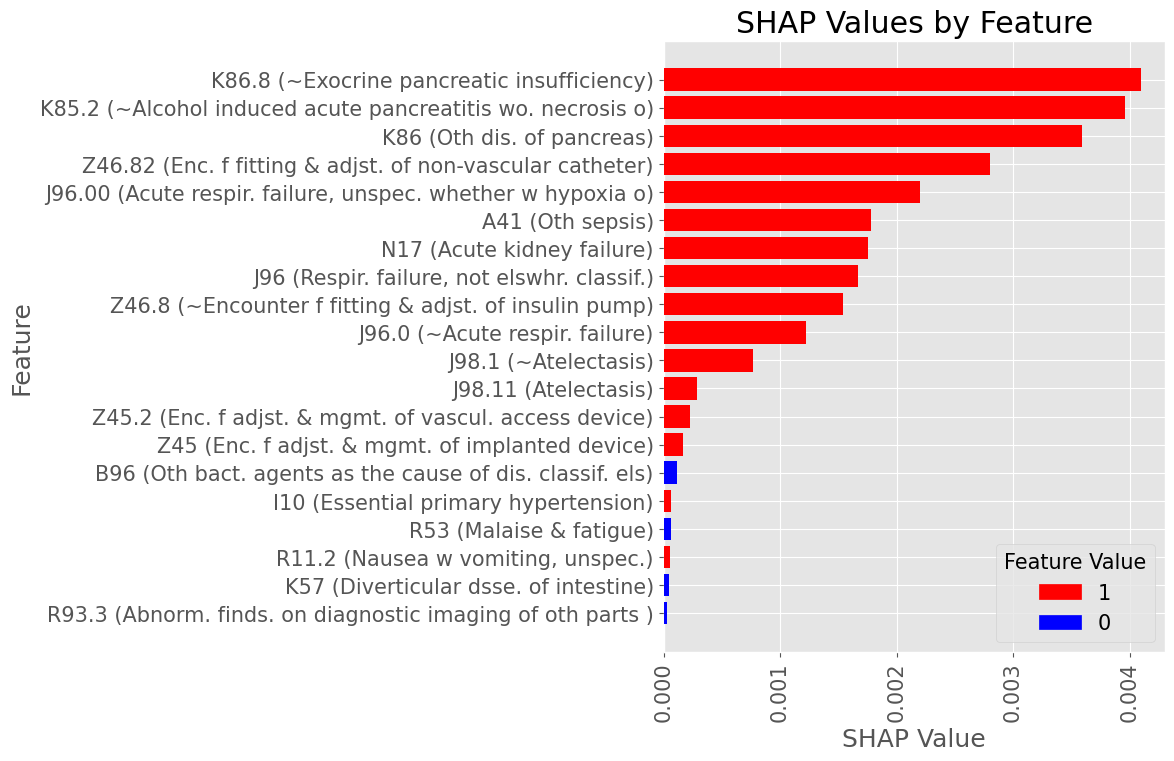
Most influential Diagnostic Codes
Male
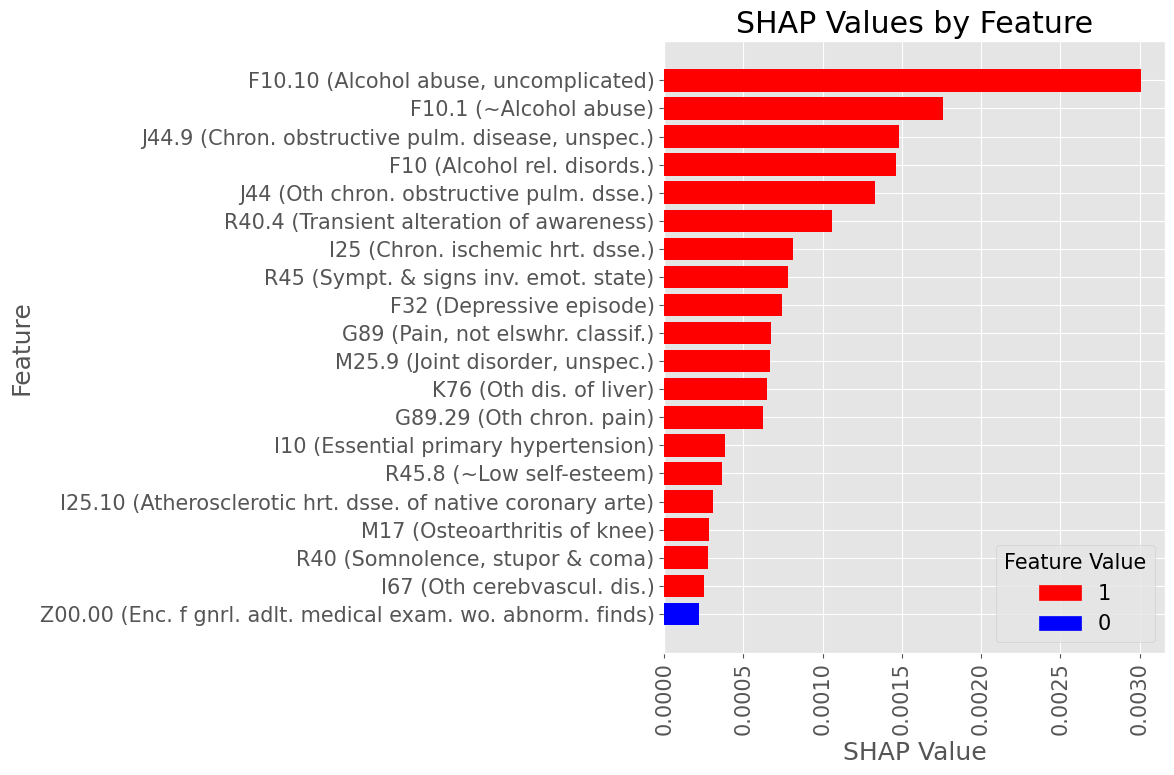
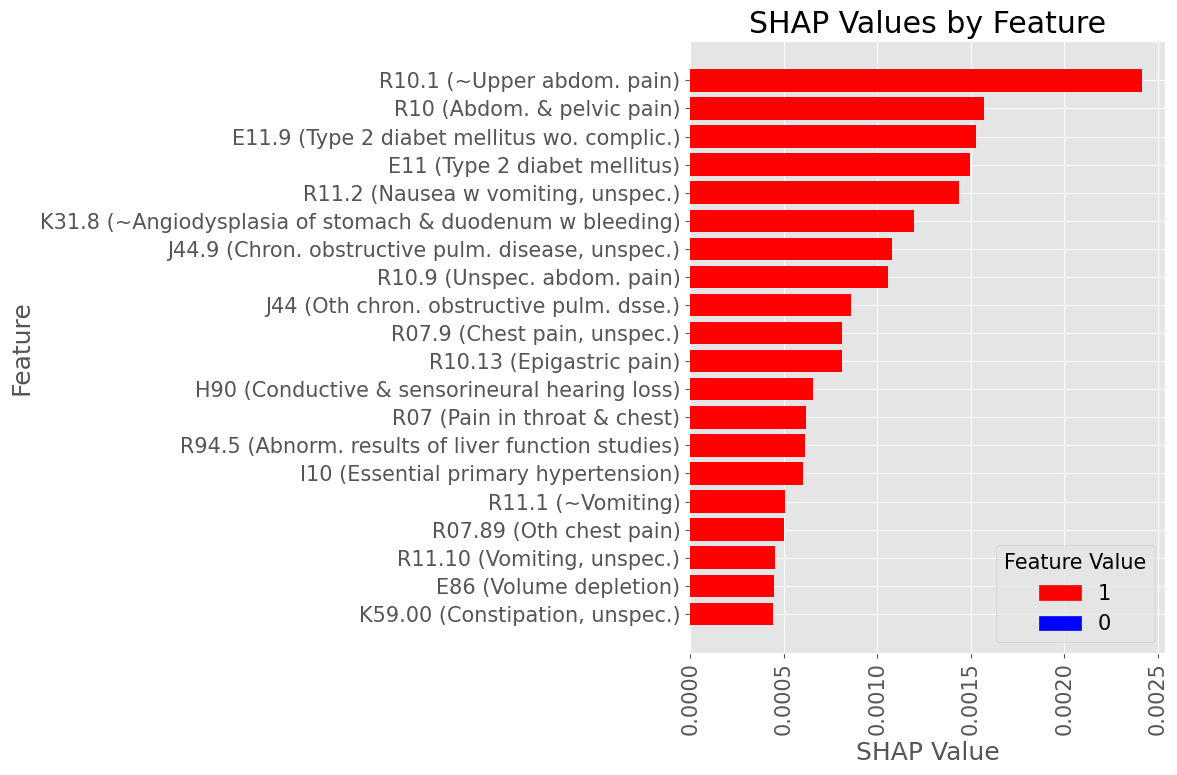
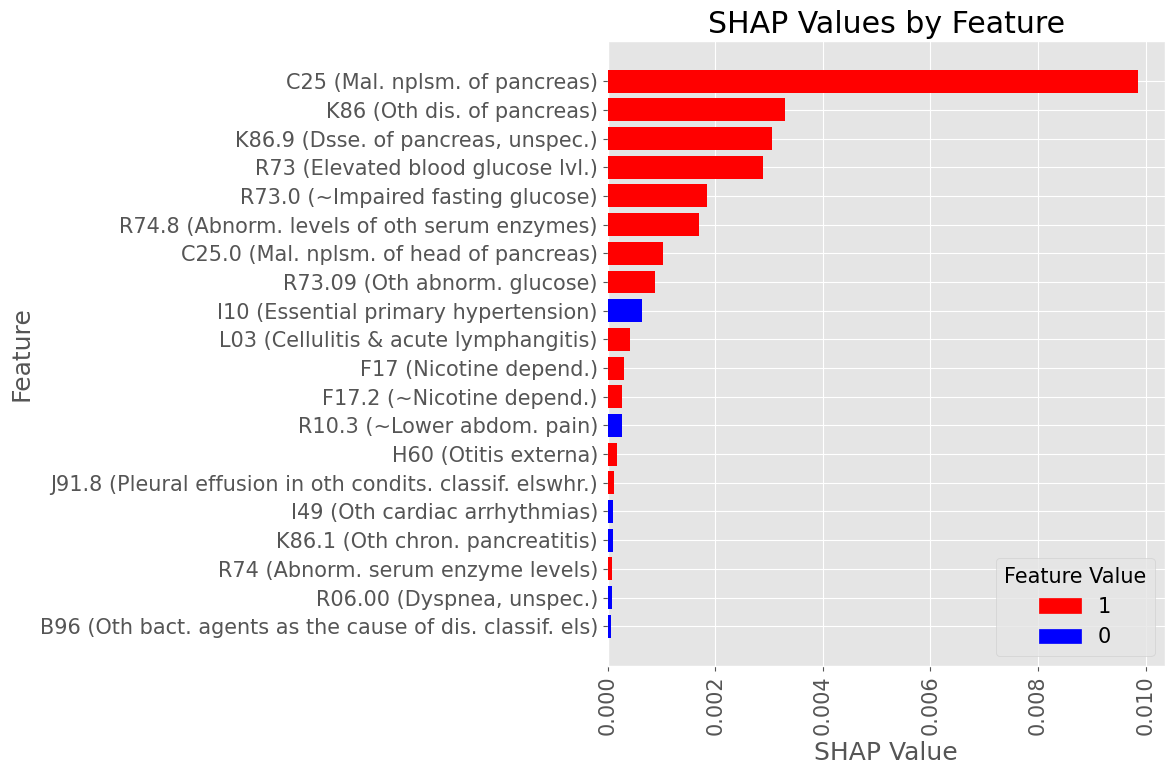
Most influential Diagnostic Codes
Female
Examples of most influential codes
Male
Examples of most influential codes
Female
Diagnoses with Highest statistically significant Log Odds by organ group
Diagnoses with Lowest statistically significant Absolute Log Odds by organ group
Subproblem 2
Progression from AP to Diabetes Mellitus
Inclusion Criteria:
Patients of any age with any K85 (Acute Pancreatitis) code recorded, with >= 1 year of records leading to the first K85 diagnosis available
Exclusion Criteria:
Patients with any Diabetes Mellitus prior to the first K85 diagnosis are excluded.
Prediction Target: Diabetes Mellitus due to Underlying Conditions (E08, E13)
Time of Prediction: Date of the first K85 diagnosis
Observation window: 1 to 2 years leading to the first K85 diagnosis
Prediction Objective: Predict if any Target diagnosis will be recorded within 2 weeks to 2 years following the first K85 diagnosis
Cohort Size:
Case: 1,329 (1.1%), Control: 122,257 (98.9%)
Males: 52,427 (42.4%), Females: 71,159 (57.6%)
Mean age at the time of prediction: 51 years 5 months
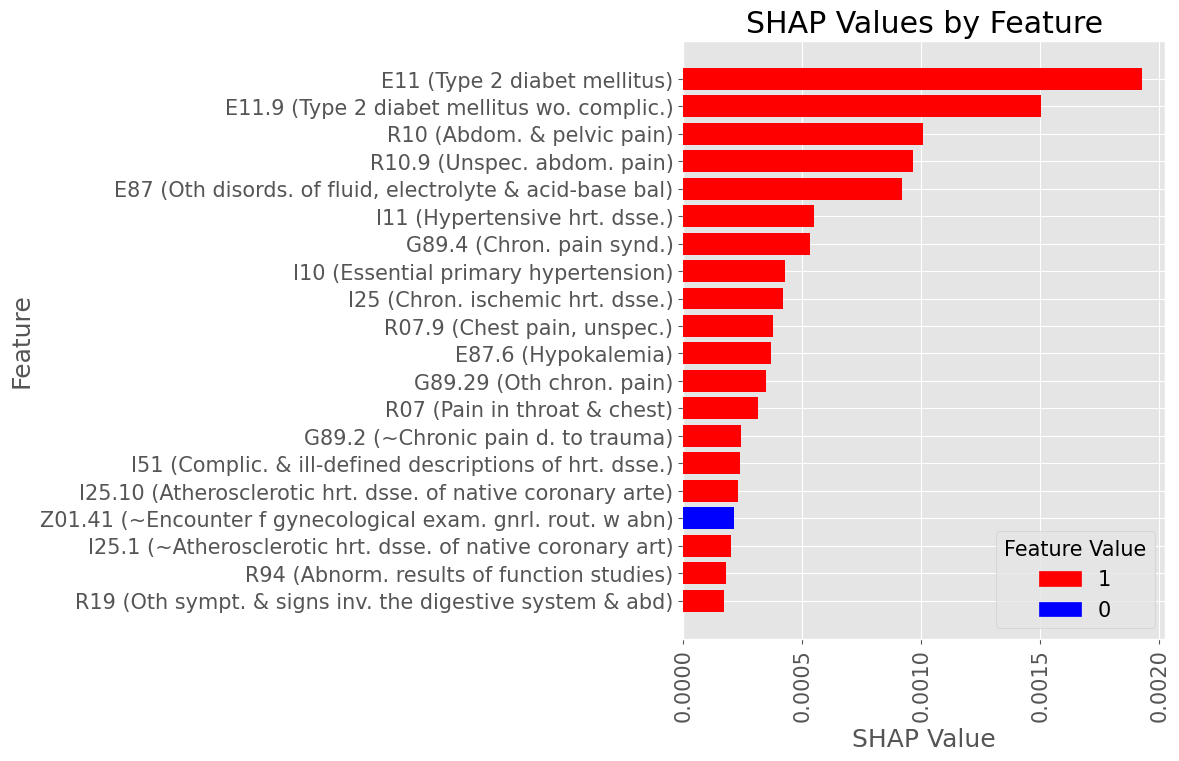
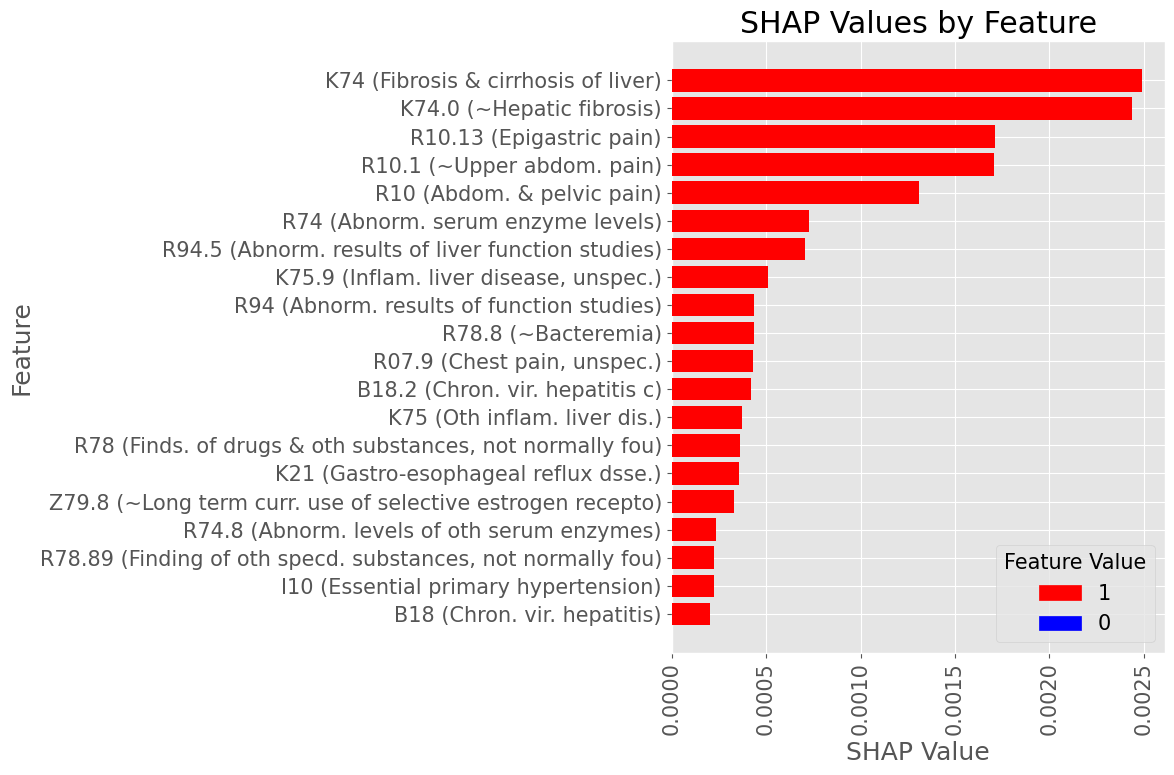
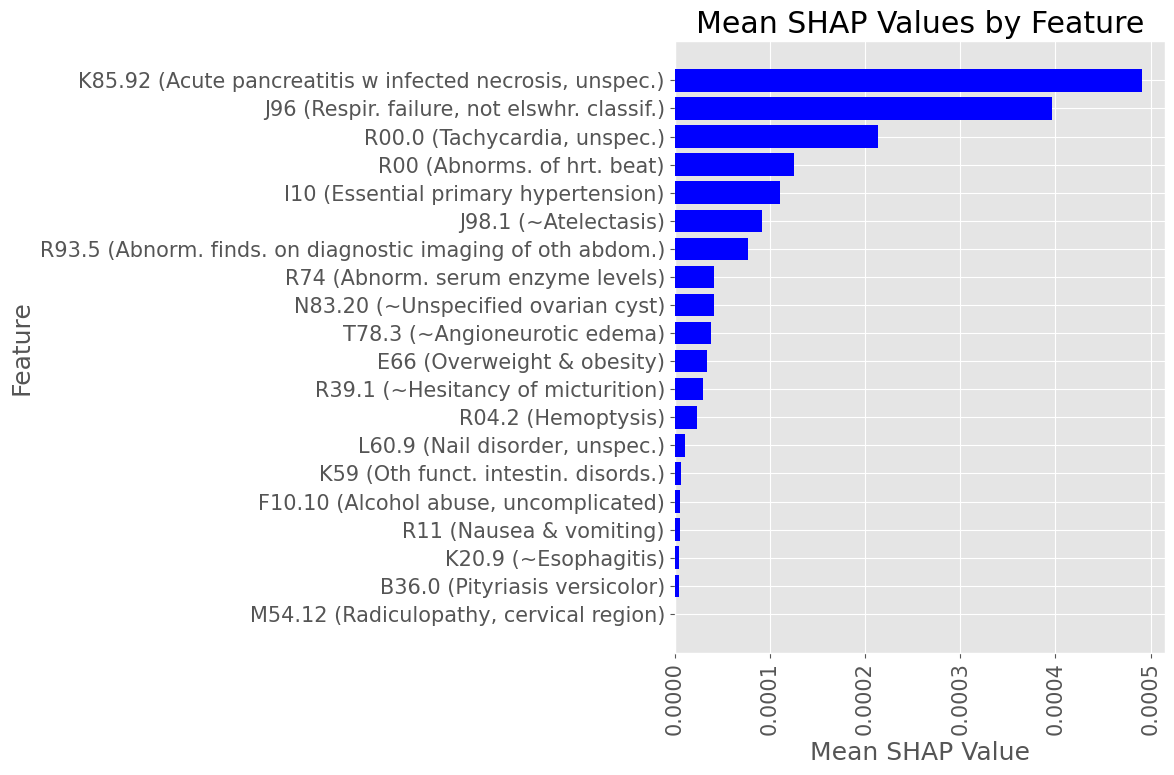
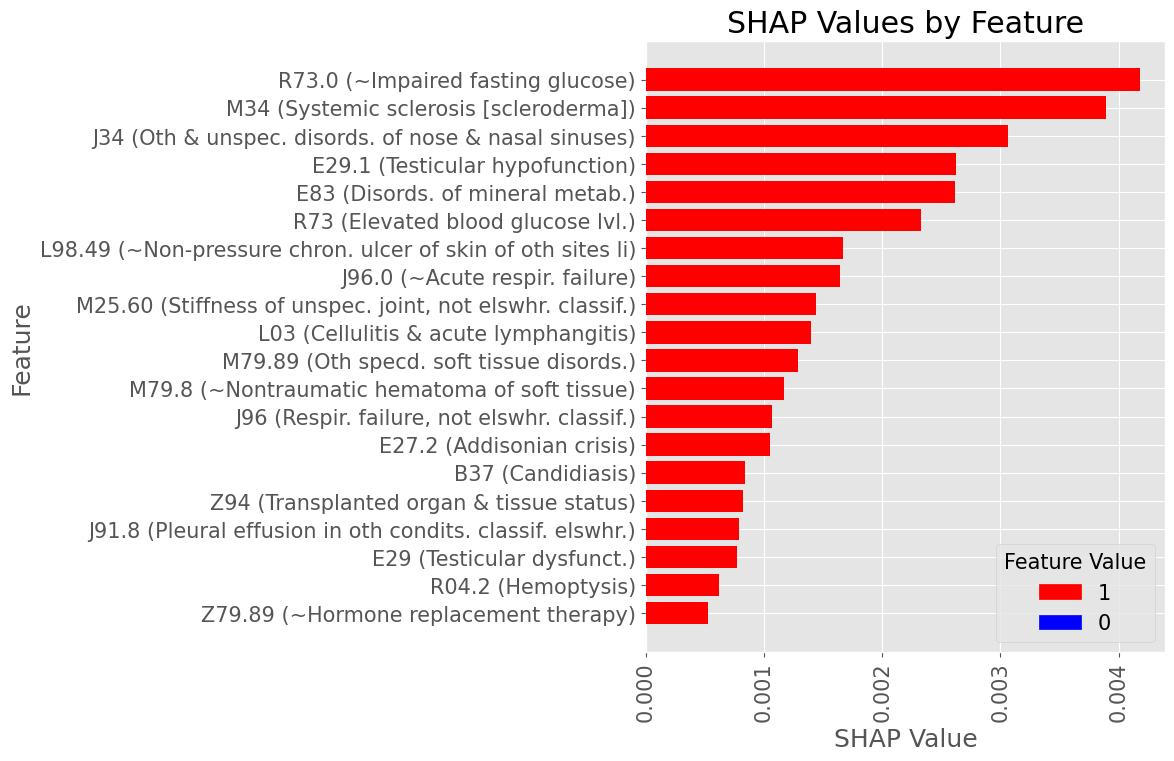
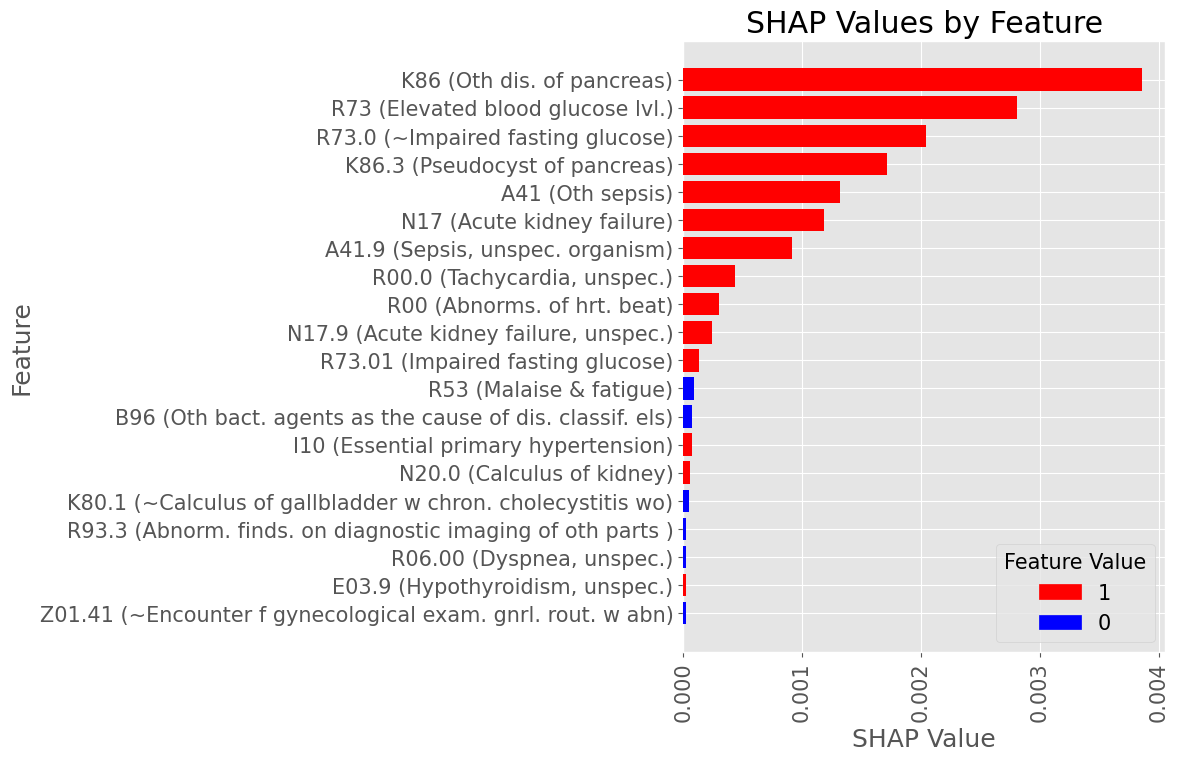
Most influential Diagnostic Codes
Male
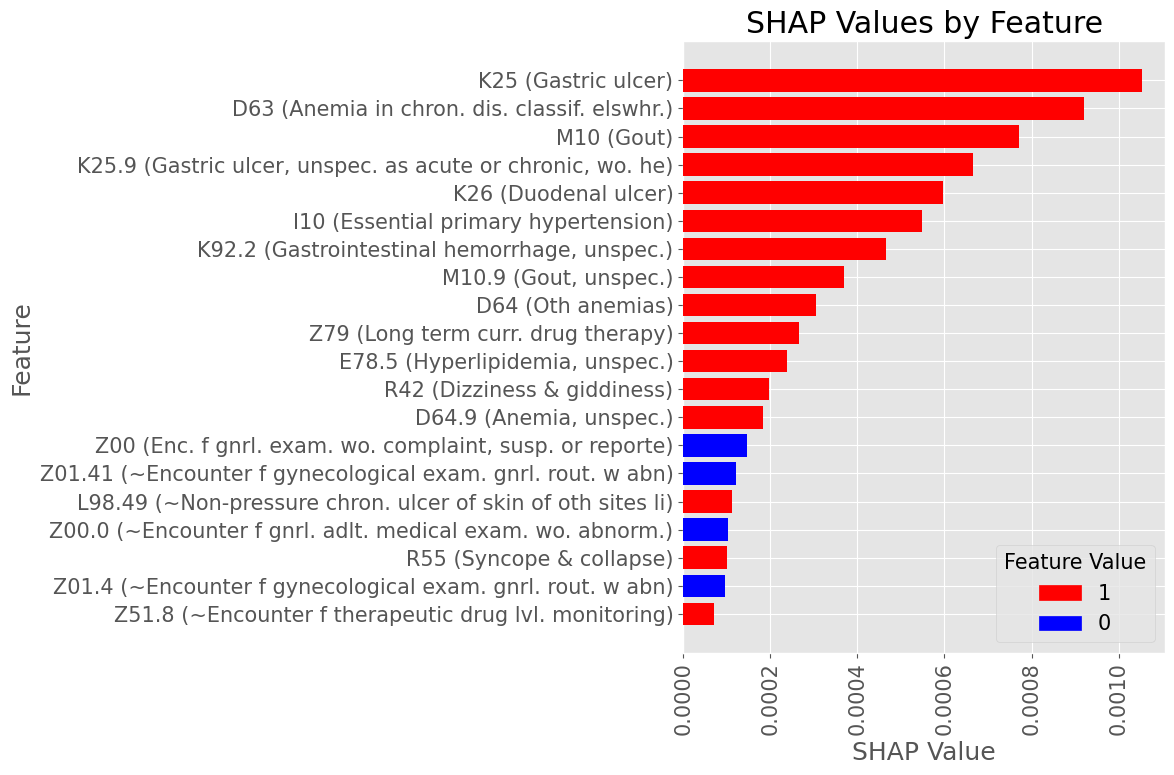
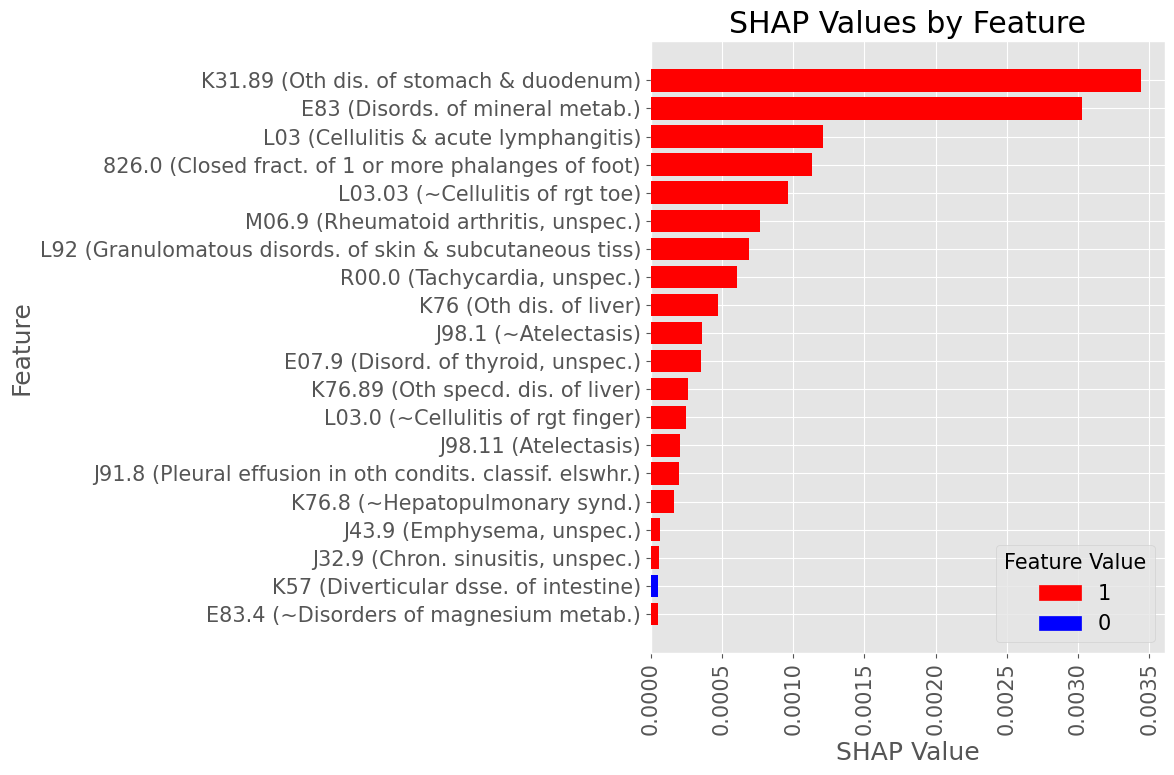
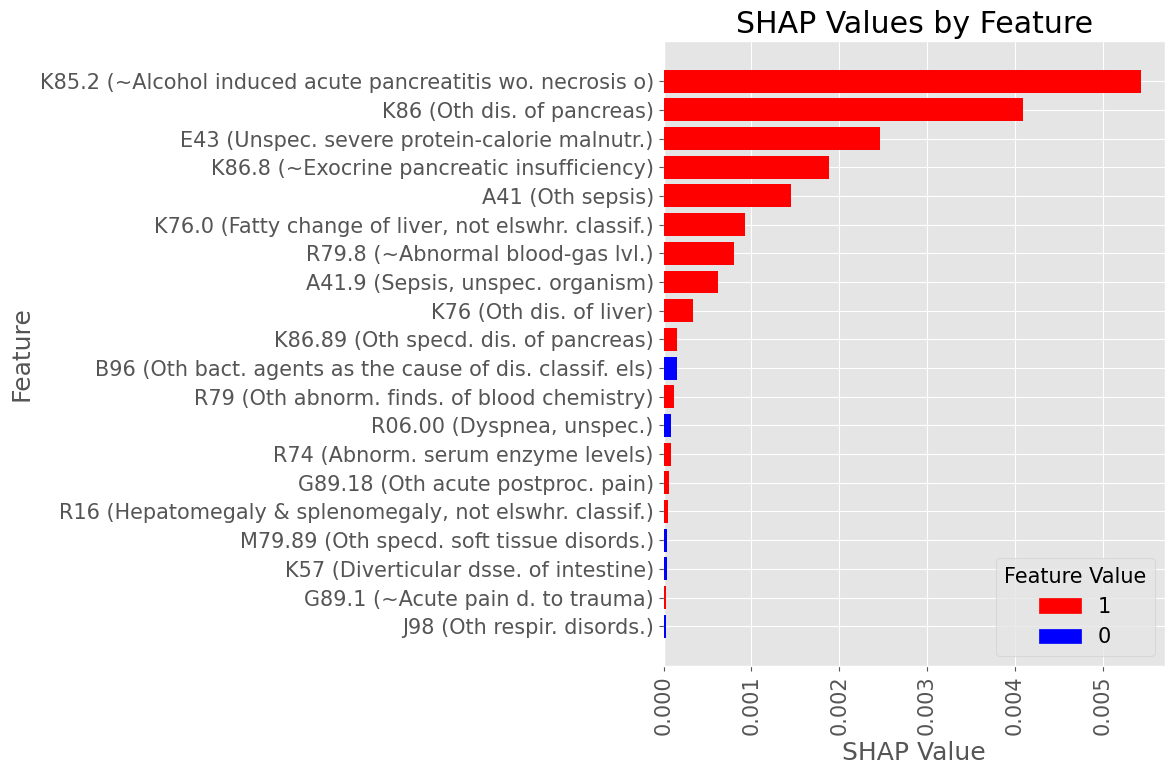
Most influential Diagnostic Codes
Female
Examples of most influential codes for True Positive patients
Male
Examples of most influential codes
Female
Diagnoses with Highest statistically significant Log Odds by organ group
Diagnoses with Lowest statistically significant Absolute Log Odds by organ group
Subproblem 3
Prediction of ICU admission following AP diagnosis
Closest matches, found in the inpatient admission services data:
Place of Service (STDPLAC) -
20 Urgent Care Facility
23 Emergency Room - Hospital
27 Inpatient Long-Term Care (NEC)
41 Ambulance (land)
42 Ambulance (air or water)
Service Sub-category Code (SVCSCAT) -
10120 Facility IP Non Acute ER
10420 Facility IP Surgical ER
10520 Facility IP Medical ER
20120 Physician Specialty IP ER
21120 Physician Specialty OP ER
21220 Physician Non-Specialty OP ER
22320 Professional OP ER
Procedure Group (PROCGRP) -
111 Emergency department visits
114 ER visits, other
Provider Type (STDPROV) -
1 Acute Care Hospital
5 Ambulatory Surgery Centers
6 Urgent Care Facility
265 Critical Care Medicine
270 Endocrinology & Metabolism
275 Gastroenterology
565 Surgical Critical Care
Closest matches, found in the Procedural codes catalog:
99291: CRITICAL CARE, EVALUATION AND MANAGEMENT OF THE CRITICALLY ILL OR CRITICALLY INJURED PATIENT;
G0390: TRAUMA RESPONSE TEAM ASSOCIATED WITH HOSPITAL CRITICAL CARE SERVICE
G0508: TELEHEALTH CONSULTATION, CRITICAL CARE, INITIAL , PHYSICIANS TYPICALLY SPEND 60 MINUTES COMMUNICATING WITH THE PATIENT AND PROVIDERS VIA TELEHEALTH
G0509: TELEHEALTH CONSULTATION, CRITICAL CARE, SUBSEQUENT, PHYSICIANS TYPICALLY SPEND 50 MINUTES COMMUNICATING WITH THE PATIENT AND PROVIDERS VIA TELEHEALTH
G9657: TRANSFER OF CARE DURING AN ANESTHETIC OR TO THE INTENSIVE CARE UNIT
By Ishanu Chattopadhyay



